A 61 year old female with hypoglycemia
This is an online e-log platform to discuss case scenario of a patient with their guardians permission.






I have been given this case to solve in an attempt to understand the topic of patient clinical data analysis to develop my competency in reading and comprehending clinical data including histoty, clinical findings, investigations and come up with a diagnosis and treatment plan..
CASE:
A 61 year old female who is resident of narketpally, came to OPD on 21st november at 12am with.
Chief complaints of:
- stiffness of muscles of hands and neck
- slurred speech
- deviation of mouth towards right.
History of present illness:
Patient was apparently asymptomatic 10yrs back and then she developed faintness, numbness and tingling sensation, burning sensation of hands and foot espcially during night and was diagnosed with Diabetes Mellitus for which she is on medication. 8months back she developed neck pain, headache, leg pain, body pains and was diagnosed with Hypertension for which she is on medication but irregularly. 10 days back she developed fever, vomitings and weakness for which she went to local area hospital and she got relieved on medication. She is also having burning micturition.From 2 days ago she was taking DM medication without intake of food and at last night she suddenly developed altered sensorium and came to hospital.
Past illness:
She is a known case of DM since 10yrs and HTN since 8months.
No H/o asthma, TB, epilepsy, CAD, CVA, Thyroid.
Treatment history:
Tab. Rabeprazole
Tab. Ondansetron
Tab. Drotaverin HCl and Mefenamic acid
Tab. Pan 40
Tab. Atenolol
Tab. Metformin HCl and Glimeperide
Syrup Liquid paraffin
Syrup Sucrafil
Disodium hydrogen citrate liquid
Tab. Nifedipine
Family history: not significant.
Personal history:
Diet: mixed
Appetite: decreased
Sleep: Inadequate
Bowel and bladder: irregular
Addictions: no
Allergies: no
General Examination:
Patient is conscious, coherent and cooperative.
Well oriented to time, place and person.
Moderately built and well nourished.
Pallor: present
Icterus: no
Cyanosis: no
Clubbing of fingers: no
Lymphadenopathy: no
Pedal oedema: no
Vitals:
BP: 130/90mmHg
PR: 68 bpm
RR: 16 cpm
SpO2: 96%
GRBS: 39 mg/dl
Systemic Examination:
CNS examination:
Patient is conscious, coherent and cooperative.
Speech is normal.
Cranial nerves: intact
Motor system:
Tone:
Right Upperlimb - Normal
Left Upperlimb - Normal
Right Lowerlimb - Normal
Left Lowerlimb - Normal
Power:
Right Upperlimb - 5/5
Left Upperlimb - 5/5
Right lowerlimb - 5/5
Left lowerlimb - 5/5
Reflexes:
Right Left
Biceps 2+ 2+
Triceps 2+ 2+
Supinator 2+ 2+
Knee 2+ 2+
Ankle 2+ 2+
Sensory system:
Right left in
Touch: N N
Temperature: N N
Pressure: N N
Pain: N N
Vibration: N N
Glasgow scale: E4 V5 M6
Cerebellar signs:
Finger nose incordination: no
Knee heel incordination: no
CVS examination:
S1, S2 are heard.
No murmurs.
Respiratory system examination:
Inspection: Chest is moving bilaterally symmetrical. No pulsations.
Palpation: Trachea is central in postion.
Percussion: Resonant sound is seen.
Auscultation: Breath sounds are vescicular.
Abdomen examination:
Inspection: Shape is scaphoid.
Movements are equal.
Palpation: No tenderness
Normal temperature
No organomegaly.
Percussion: Normal.
Auscultation: Bowel sounds are heard.
Provisional diagnosis:
- Oral Hypoglycemic Agent induced Hypoglycemia.
- Prerenal AKI.
Investigations:
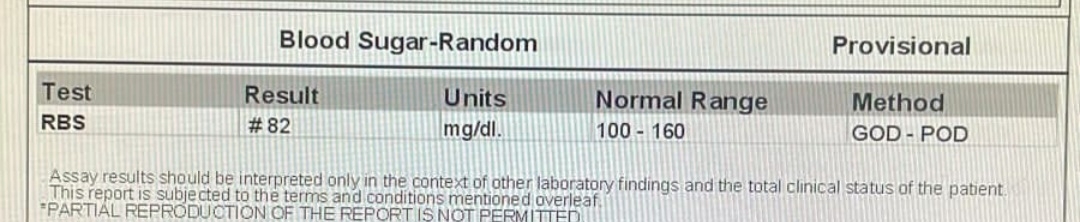
Random Blood Sugar:
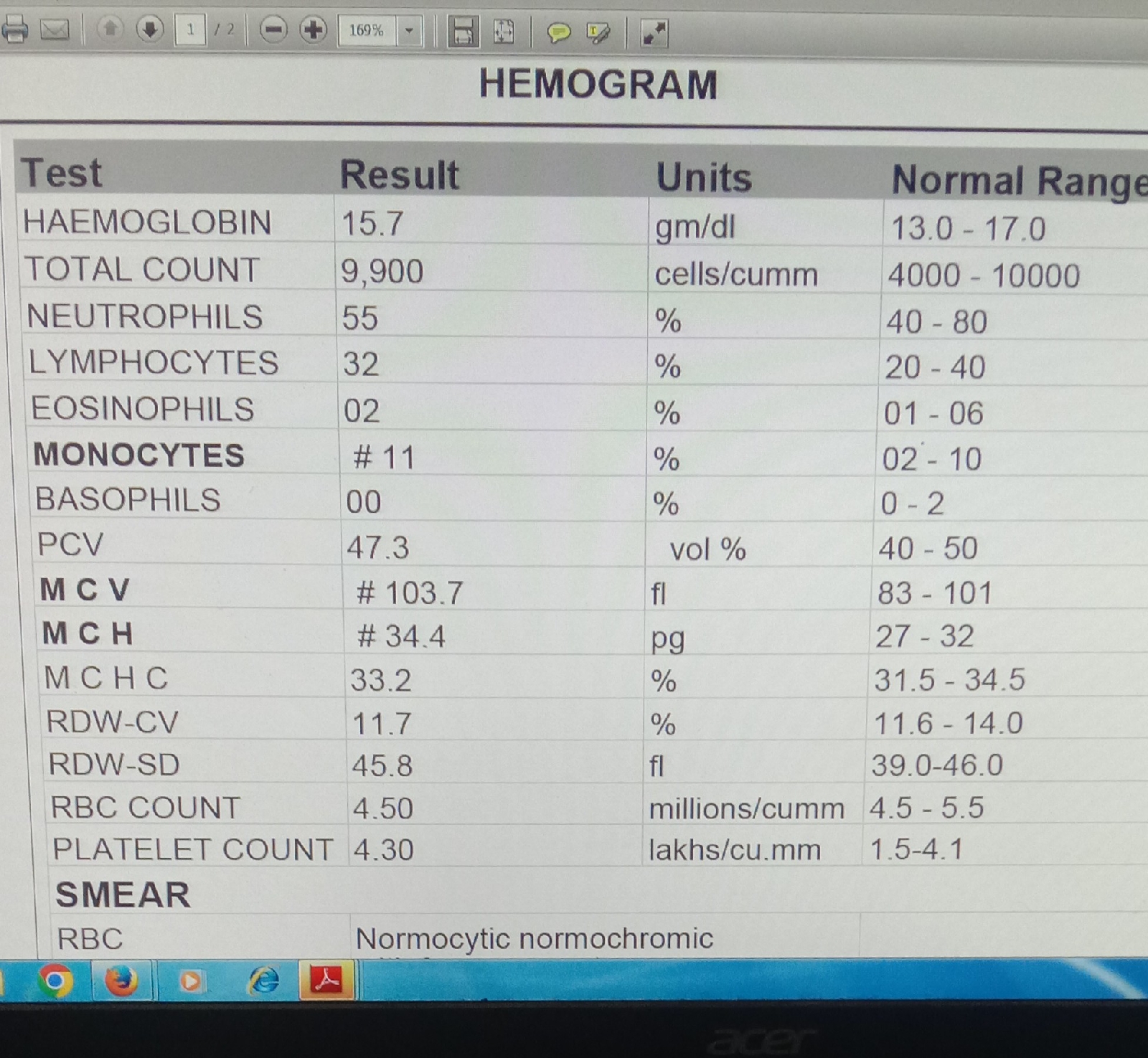
Hemogram:
Complete Urine Examination:
RFT:
APTT:
Prothrombin Time(PT):
ECG:
Final diagnosis:
RECURRENT HYPOGLYCEMIA ( SECONDARY TO OHA INDUCED ) RESOLVED
IDA ? SECONDARY TO ? NUTRITION
? PRE RENAL AKI ON CKD
DIABETIC RETINOPATHY
GASTROPERESIS
NEUROPATHY
TREATMENT:
1. INJ HAI SC/ TID
2.INJ NPH SC/ BD
3.TAB PREGABALIN 75 mg
4.SYRUP CREMAFFIN 15 ml
5.TAB MET XL 12.5 MG