50 year old female with fever
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.
A 50 year old female patient agricultural labourer by occupation was bought to the casualty with the chief compliants of fever since 5 days
Loose stool since 1 day( 3 episodes)
Vomitings since 1 day ( 2 episodes)
HOPI.
Patient was apparently asymptomatic 5 days back then she developed fever which was high grade, intermittent in nature associated with chills and rigors and relieved on medication.patient also had a history of loose stools( 3 episodes) water in consistency . She also had history of 2 episodes of vomiting which is non bilious non projectile with food as contents.
No H/O bleeding manifestations, pain abdomen , head ache, chest pain,cough.
PAST HISTORY
No similar complaints in the past.
Not a known case of diabetes, Hypertension,asthama, epilepsy tuberculosis,CAD,CVA.
FAMILY HISTORY: Her son had similar history and got admitted yesterday.
PERSONAL HISTORY
DIET: mixed.
APPETITE: NORMAL
SLEEP: adequate
BOWEL AND BLADDER MOVEMENTS: regular
No addictions
No allergies.
ON GENERAL EXAMINATION
patient is conscious, coherent,co operative well oriented to time, place and person, moderately built and moderately nourished
AFEBRILE
Bp:110/70 mm hg
PR:86bpm
RR;16cpm
Spo2:96% at room air
GRBS:293mg%
Physical Examination:
Pallor:absent
Icterus: absent
cyanosis: absent
clubbing : absent
lymphadenopathy:absent
pedal edema: absent
SYSTEMIC EXAMINATION:
CVS
S1 and S2 are heard
No thrills
No murmurs
RESPIRATORY SYSTEM
INSPECTION:
Tracheal position is central
Symmetrical chest
PALPATION:
All inspectory findings are confirmed by palpation
Trachea is central
Chest is symmetrical
Symmetrical expansion of chest.
PERCUSSION:
Resonant on percussion.
AUSCULTATION:
Breath sounds are normal.
PER ABDOMEN
Shape : scaphoid
Tenderness : Present
No palpable mass
Hernial orifices : Normal
No free fluid
No bruits
Bowel sounds : present
CNS
Conscious
Speech : Normal
No signs of meningeal irritation
Cranial nerves : intact
Motor system : Normal
Sensory system : Normal
Reflexes : Normal.
INVESTIGATIONS:
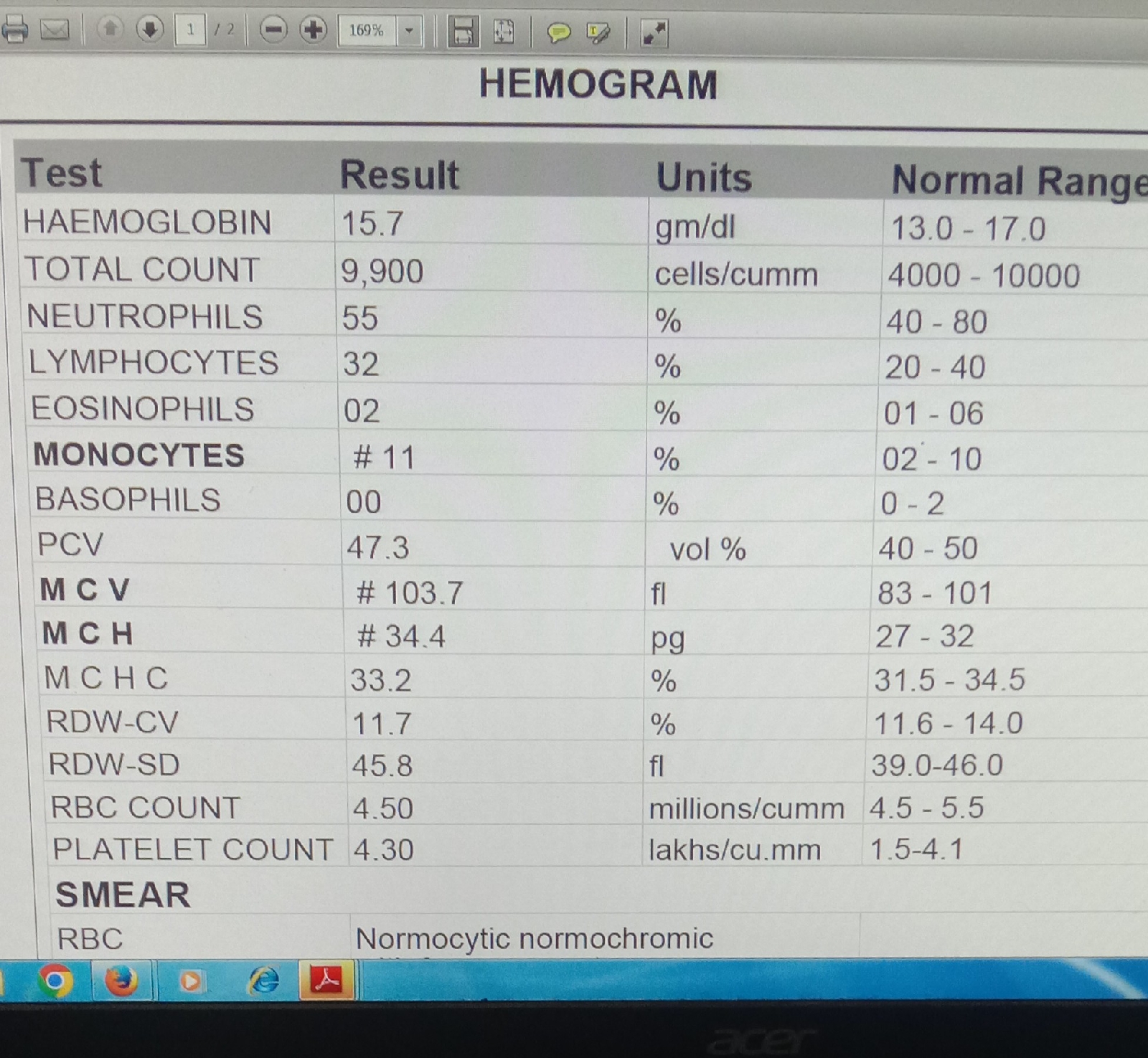
HEMOGRAM.
HB:12.8
TLC:2000
PCV:39.3
PLT:30,000
SEROLOGY: NEGATIVE.
APTT: 33 sec
BLEEDING TIME: 2 min 30 sec
CLOTTING TIME: 4 min 30 sec
RBS:114
BLOOD UREA:. 38
NS1 : POSITIVE.
TOTAL BILURUBIN:0.69
DIRECT BILIRUBIN:0.18
SGOT;79
ALP:133
SGPT:28
TOTAL PROTIEN:5.5
AlBUMIN:3.3
PROTHROMBIN TIME:16 sec
INR:1.11
SERUM CREATININE:0.9
SODIUM:138
POTASSIUM:4
CHLORIDE:102
STOOL FOR OCCULT BLOOD - POSITIVE
PROVISIONAL DIAGNOSIS
VIRAL PYREXIA (? DENGUE FEVER)
TREATMENT
1.ivf ( 2 NS,1 RL@ 100 ML/HR)
2.INJ NEOMOL 1 GM IV/BD( IF TEMP> 101F)
3.TAB DOLO 650 MG / TID.
TAB ZOFER 4 MG PO/SOS.
5.MONITOR VITALS 2ND HRLY